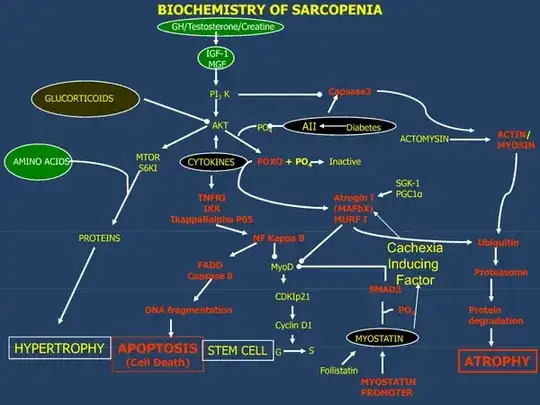
Morley (2016) states (with more references than I am copying across here),
At a basic level, protein synthesis and/or degradation are controlled by activation of the insulin or IGF-1 receptor.
...
The primary treatment of sarcopenia is resistance exercise. As was shown by the LIFE study (Pahor, et al. 2014), aerobic exercise can also decrease functional decline in lower limb muscles. Exercise has also been shown to be an important therapeutic approach to reversing frailty. There is evidence to support that excess protein [1–1.2 g (kj day)] may also enhance muscle mass and, to a lesser extent, function (Bauer, et al. 2013). This is particularly true for leucine enriched essential amino acids (whey protein). Essential amino acid supplementation prevents muscle mass loss due to bed rest. A recent multicenter study has shown that whey protein together with vitamin D increased both muscle mass and stair climb. There is some evidence for synergistic effects of exercise and protein to enhance muscle function. Vitamin D supplementation increases muscle strength without increasing muscle mass or power. Vitamin D is more effective in older persons and those with low vitamin D levels. It also decreases falls in persons who are vitamin D deficient. At present, no drugs have been shown to be clinically more therapeutically effective.
For exercise and diet there is the following from Waters, et al. (2010)
With exception of ACEI as a pharmaceutical intervention, the most compelling evidence to combat sarcopenia is resistance training either alone or in combination with nutritional supplements.
For anabolic steroids/SARMs, Morley (2016), states that with:
- Nandrolone
there is no evidence that it increased strength
- MK0773 (TFM-4AS-1)
a 4-aza steroidal drug that has androgen gene selectivity. In females, it increased IGF-1 as well as stair climbing power and gait speed (Papanicolaou, et al. 2013). This study was terminated because of an increased signal for cardiac failure. In women with sarcopenia, it increased muscle mass, bilateral leg press, and stair climbing power but not gait speed (www.clinicaltrials.gov). The study in males was reported at the 90th Endocrine Society in 2008. It showed anabolic effects of MK0773.
- Enobosarm
In a 12-week study, increased total lean mass and stair climb (Dalton, et al. 2011). In female patients with cancer, enobosarm increased lean mass compared to baseline, but not significantly compared to placebo
Overall, these studies of SARMs have shown no advantage over testosterone.
- Growth Hormone/Insulin Growth Factor-1
Increased nitrogen retention and increased muscle mass
- Ghrelin antagonists
Overall, while ghrelin agonists will increase food intake and muscle mass, it is unlikely that they will produce a significant effect on function in persons with sarcopenia.
- Myostatin antibodies
Increased lean body mass and handgrip
- Activin 11R antagonists
Increased thigh muscle volume, muscle mass, and 6-min walk distance
- Angiotensin converting enzyme inhibitor (perindopril)
Increased distance walked and decreased hip fracture
- Espindolol (B1/B2/B3 adrenergic receptor antagonist)
Maintains muscle mass and increased hand grip strength
- Fast skeletal muscle troponin activators (Tirasemtiv)
Improves muscle function
References
Bauer, J., Biolo, G., Cederholm, T., Cesari, M., Cruz-Jentoft, A. J., Morley, J. E., ... & Visvanathan, R. (2013). Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. Journal of the american Medical Directors association, 14(8), 542-559.
PMID: 23867520 DOI: 10.1016/j.jamda.2013.05.021
Dalton, J. T., Barnette, K. G., Bohl, C. E., Hancock, M. L., Rodriguez, D., Dodson, S. T., ... & Steiner, M. S. (2011). The selective androgen receptor modulator GTx‐024 (enobosarm) improves lean body mass and physical function in healthy elderly men and postmenopausal women: results of a double‐blind, placebo‐controlled phase II trial. Journal of cachexia, sarcopenia and muscle, 2(3), 153-161.
PMID: 22031847 PMCID: PMC3177038 DOI: 10.1007/s13539-011-0034-6
Morley, J. E. (2016). Pharmacologic options for the treatment of sarcopenia. Calcified tissue international, 98(4), 319-333.
DOI: 10.1007/s00223-015-0022-5
Pahor, M., Guralnik, J. M., Ambrosius, W. T., Blair, S., Bonds, D. E., Church, T. S., ... & King, A. C. (2014). Effect of structured physical activity on prevention of major mobility disability in older adults: the LIFE study randomized clinical trial. Jama, 311(23), 2387-2396.
PMID: 24866862 PMCID: PMC4266388 DOI: 10.1001/jama.2014.5616
Papanicolaou, D. A., Ather, S. N., Zhu, H., Zhou, Y., Lutkiewicz, J., Scott, B. B., & Chandler, J. (2013). A phase IIA randomized, placebo-controlled clinical trial to study the efficacy and safety of the selective androgen receptor modulator (SARM), MK-0773 in female participants with sarcopenia. The journal of nutrition, health & aging, 17(6), 533-543.
PMID: 23732550 DOI: 10.1007/s12603-013-0335-x
Waters, D. L., Baumgartner, R. N., Garry, P. J., & Vellas, B. (2010). Advantages of dietary, exercise-related, and therapeutic interventions to prevent and treat sarcopenia in adult patients: an update. Clinical Interventions in aging, 5(1), 259—270.
PMCID: PMC2938033